Episode Description: Continuing from our previous episode where we began exploring the idea of Cannabis as medicine, in this episode we dive into exploring how medical claims are derived, what it takes to develop a Cannabis-based drug in the United States, and what outcomes health care professionals are seeing in their patients that are using Cannabis as a medicine.
TRANSCRIPT
You’re listening to the Curious About Cannabis Podcast
Before we get started let me share a little disclaimer here. In this episode we are going to be discussing the medical uses of Cannabis. All of the information I present to you in this podcast is for education and entertainment purposes only and should not be considered medical advice. Never make decisions about your health based on anything you hear me or any other podcast host talk about. I’m simply sharing information that I’ve collected from talking with professionals with relevant experience or from research studies that are available. But I’m not a doctor, and you should always get your medical advice from a licensed health care professional. Now with that out of the way, let’s move on.
[INTRO SEGMENT]
In the previous episode of the podcast we began exploring the concept of Cannabis as medicine. We looked at many of the ways in which Cannabis has been used as a medicine in the past, and some ways in which Cannabis based pharmaceuticals are being used as medicines today. Picking up where we left off, I wanted to explore the ways in which medical claims are derived. How do we determine that something is a medicine? And what results are clinicians seeing in their patients that are using Cannabis?
[INTRO MUSIC]
Hey everybody, this is Jason Wilson with the Curious About Cannabis Podcast, thanks so much for tuning in once again.
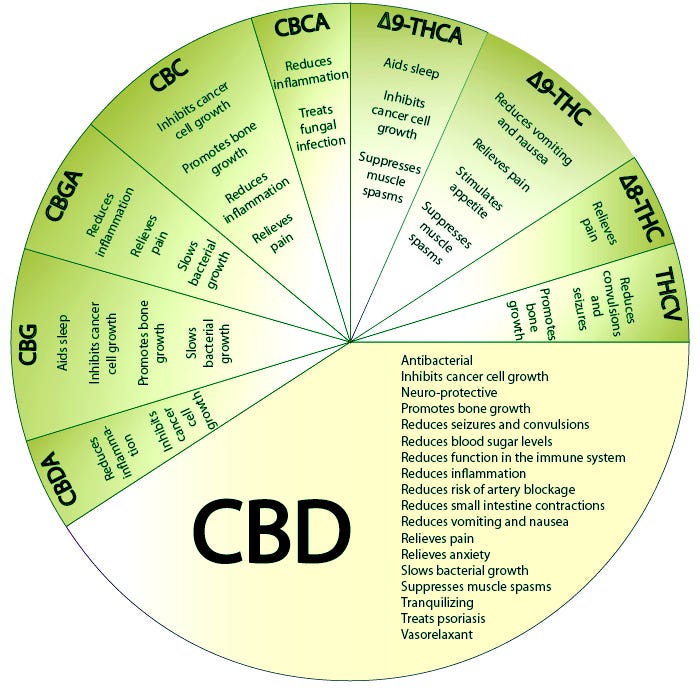
As we covered in the previous episode, there are a lot of medical claims swirling around Cannabis. If you go into just about any Cannabis dispensary, you are likely to see posters on the wall indicating the myriad of different chemicals in Cannabis and their supposed effects.[1] [2] However, many times these kinds of charts are built off of very simple, pre-clinical research data, that may not have any relevance in a real-life Cannabis use scenario.
How are medical claims derived?
So, how are medical claims derived?
There are several forms of medical research of varying degrees of quality.[3] On one end of the spectrum are anecdotal reports – these are basically eye-witness testimonies from a single person or small group of people. Up from that you have case studies, usually written by a professional describing an incident in detail. Moving along, there are observational studies, where a health care professional watches a patient engage in an activity and records the outcomes. On the other far end of the spectrum is the gold standard of randomized controlled trials.[4]
When a drug is being developed, typically the first way it is studied is through in vitro research.[5] In vitro studies are laboratory studies performed in test tubes or petri dishes. In vitro literally means, “in glass”.
[JUSTIN FISCHEDICK]
This is Justin Fischedick. Justin is a natural products researcher that studies the activity of the chemical constituents of plants, including Cannabis.
[JUSTIN FISCHEDICK]
Then there are in vivo studies, which are in living animals.[6]
[JUSTIN FISCHEDICK]
But there are limitations to each of these types of studies, and the results of an in vitro study or an in vivo animal study cannot always be easily extrapolated to real-life human clinical situations.[7]
[JUSTIN FISCHEDICK]
I had a conversation with cellular and molecular biologist, Dr. Anthony Smith, about this issue regarding the limitations of animal studies.[8]
[ANTHONY SMITH]
A lot of Cannabis research has, up to a point, been primarily in vitro and in vivo rodent studies, but very few research projects with Cannabis have crossed into the world of placebo controlled double blind clinical trials with large patient populations, and many politicians and regulatory bodies continue to claim that because of this lack of clinical trial data, herbal Cannabis or Cannabis products cannot be deemed safe or a viable medicine for a condition.
Let’s break this phrase down. “Placebo controlled” refers to the fact that a compound is given to some of the patients in a trial which is intended to have no effect. In general, it is expected that if something is a candidate to be considered a medicine, it needs to perform better than a placebo. It can be difficult to adequately utilize a placebo in a THC-rich Cannabis study. Because THC has such distinct effects, it is pretty difficult to fool people into thinking they got the drug when they actually did not. This is referred to as “incomplete blinding” because the patients are not truly blinded to whether they received the drug or not. The gold standard for clinical trials is for a study to be “double blind”.
“Double blind” refers to the idea that both the clinician performing the study, and the patients participating in the study, are blind to whether they received the research drug, or the placebo. This is important because there are various biases that can enter a study if the physician knows who has had the placebo or not, and likewise, patients may react differently in a study if they know they are receiving a placebo – although some modern research is beginning to call this idea into question.
Lastly, large sample sizes are required in order to understand whether the results of a clinical trial are representative of a larger population.[9] A study that only examines the response of a couple dozen or even a couple hundred people is really small, and can’t really represent the hundreds of millions of people living in the United States, much less the billions of people living in the world.
There’s also the issue of repeatability that is worth mentioning. Even if a research study is placebo-controlled and double blinded with a good sample size – it is still important that the study be replicated by another set of researchers, in another location, with a different population of people. Research findings are much more robust when they have been repeated.[10] There is always the chance that there are some variables unaccounted for in a study that could explain the results differently than what the researchers were focused on.
When trying to interpret medical research, there is also the issue of deciphering what the clinical studies are trying to measure, and whether the significant effects that are identified in a study are relevant in a real-life clinical setting. This is the issue of statistical significance vs clinical significance.[11] Statistical significance is a measure of the likelihood that a result is not due to pure chance. Whereas clinical significance is a measure of the practical significance of a treatment in a clinical setting. Basically, just because a research study determines that something exhibits an effect that is statistically significant, it doesn’t mean that the effect will end up being significant in any practical sense when someone consumes that thing.
There is another similar issue also facing drug development and medical research, and that’s the battle between efficacy research and effectiveness research.[12]
[JASON MILLER]
So we’ve established that there are a lot of different ways to study medicine, and the results of some of these studies are not necessarily straightforward to interpret.
[ETHAN RUSSO]
All of these nuance details about research are important when it comes to the development of Cannabis based pharmaceuticals. To get a drug approved as a medicine in the United States, a company has to present lots of data that shows that the drug, and not a placebo, provide an intended therapeutic effect for a particular condition or set of conditions.[13] That takes a lot of time, a lot of energy, and a lot of money.
[ETHAN RUSSO]
Sativex, or Nabiximols as it is also known, is a particularly interesting drug to focus our attention on. Sativex is a mouth spray that consists of a standardized Cannabis extract with a 1:1 ratio of CBD to THC.[14] Unlike Epidiolex[15], which is often criticized for being an isolated cannabinoid drug like Marinol[16] – Sativex consists of a wide diversity of plant compounds extracted from Cannabis. This means that the clinical data on Sativex is likely to be more relevant when thinking about the therapeutic potential of herbal Cannabis or Cannabis extracts, than research on isolated THC, like Marinol, or CBD, like Epidiolex.
[ETHAN RUSSO]
Dr. Russo makes a great point here. Just because cannabinoid and Cannabis-based pharmaceuticals are being developed, it doesn’t mean that herbal Cannabis and the use of Cannabis extracts is going away anytime soon.
And in fact, many people tend to prefer the use of herbal Cannabis or Cannabis extracts for a number of reasons. Sometimes it’s efficacy related, but sometimes it’s cost related. Pharmaceuticals can be extremely expensive.[17] When you can grow a plant at home and can easily make your own extract with as good or better efficacy than a pharmaceutical, it’s pretty hard to justify going the pharmaceutical route. However, pharmaceuticals are standardized and very consistent batch to batch. It’s possible that trying to treat a condition with homegrown Cannabis or black market (or even legal medical or recreational) Cannabis may not provide consistent outcomes because the products’ chemistry will be different batch to batch.
Unfortunately, there is really not much research available regarding herbal Cannabis or Cannabis extracts. This is for multiple reasons. One reason is that research tends to happen with products that can be patented. So, there is not a huge financial incentive to do expensive research on herbal Cannabis or unstandardized Cannabis extracts. Another issue is that Cannabis flower and extracts are very diverse and inconsistent in their chemistry batch to batch.
What are clinicians seeing in patients using Cannabis?
However, despite all of these issues, clinicians around the US are noticing striking results in many patients.
[JANNA CHAMPAGNE]
[JAMES TAYLOR]
All of this positive benefit that some of these health care professionals are seeing does not mean that Cannabis is without risks. For an in-depth review of the risks associated with Cannabis use, I recommend listening to the first three episodes of this season where we explored the question, “Is Cannabis Safe?”.
Cannabis can interact with other medications and it’s not for every person or every condition.
[JASON MILLER]
So despite some of the miraculous claims about Cannabis – it’s not a cure-all, and some of the claims made by advocates are overhyped. However, other clinicians I spoke with shared additional stories of the successes of the medical use of Cannabis – which begs a question – just how much evidence is required before Cannabis, or any other natural product, can be accepted as an effective medicine?
We’ve discussed that the gold standard of medical research is considered to be the randomized controlled trial – but it’s an extremely expensive process to get something through the drug approval process in the United States.[18] Because this process is so expensive, it is rare for a company to spend the millions, or sometimes billions, of dollars required to study a natural product alone that they cannot patent and capitalize on later. Additionally, natural products are challenging to standardize and control, which does not lend itself well to modern medical research schemes.
[JAMES TAYLOR SEGMENT]
We have also covered the fact that Cannabis has an extraordinarily long track record with humans, going back nearly 5000 years or more. Through that time, records of varying degrees of quality have been kept about the medical use and toxicity of Cannabis for thousands of years. The historical record indicates that Cannabis has been considered a potent medicine all the way up until the 1930s when Cannabis prohibition began. We haven’t even discussed the history of Cannabis prohibition here but let me just say – Cannabis prohibition was not backed by science, and many medical associations were unhappy when access to Cannabis was prohibited.
Modern research has confirmed that, in fact, many of the traditional medical uses of Cannabis are well-founded and, compared to many foods and drugs, Cannabis is very safe. Where we lack clinical research, we have a host of anecdotal reports, case studies, and observational studies documenting the medical efficacy of Cannabis. And while these types of research may be considered lower quality, at a point these reports become overwhelming in their results. And yet, today in 2019 in the United States, people are still struggling to get legal access to medical Cannabis.
While many of you may already be familiar with a little girl named Charlotte Figgi[19] that brought nationwide attention to the treatment of CBD-rich Cannabis for seizures in a famous CNN special with Dr. Sanjay Gupta called Weed[20], you may be less familiar with another little girl that is fighting the same fight in my home state of Mississippi, and her name is Harper Grace[21]. Harper Grace is a little girl that also suffers from seizures, similar to Charlotte. Her parents found that CBD-rich Cannabis was an effective treatment. In 2014, after a lot of advocacy from Harper Grace’s parents and friends, the state legalized CBD oil, in a limited capacity for limited conditions in a limited selection of patients. Since the law passed, which is actually named after Harper Grace, that little girl still has not been able to get access to CBD treatment, and now her parents are fighting for statewide medical marijuana legalization for 2020.
[NEWS CLIP]
This issue is especially poignant considering the countries only federally sanctioned Cannabis research and development laboratory is located at the University of Mississippi.
Let’s review what we’ve learned.
- Cannabis has been used as a medicine for a lot of different medical conditions for thousands of years.[22] Up until the early 1940s, Cannabis was even part of the US Pharmacopoeia until prohibition began.
- Medical research comes in a lot of forms, and we have to be careful not to conflate the statistical significance of an effect measured in a research study with the clinical significance of an effect measured in a therapeutic setting.
- We can’t assume anything based on a single research result. Research findings always need to be replicated by a different group of researchers.
- The clinical research that is currently available about Cannabis indicates that it could hold promise for the treatment of conditions like nausea, loss-of-appetite, chronic pain, and spasticity.[23] [24]
- There are case studies and uncontrolled clinical research that indicate that Cannabis could be useful for a number of other conditions like autism, ADHD, PTSD, anxiety, depression, and immune system related disorders. While there are numerous case studies and observational reports documenting Cannabis’ efficacy treating conditions like these in patients, it is difficult to interpret that data and extrapolate it to a much larger population.
- There’s a lot we don’t know. Cannabis comes in a lot of different forms. There are many different chemical profiles of Cannabis, each with its own therapeutic index. We are just scratching the surface with understanding Cannabis and we have a long way to go.
- We do know that Cannabis is very safe when consumed responsibly. It is impossible to lethally overdose on Cannabis and many of the adverse health risks of Cannabis can be minimized by utilizing oral forms of Cannabis at low dosages. For more information about the safety of Cannabis, check out episodes 1-3 where we explore this topic at length.
- Clinicians working with patients using Cannabis are seeing positive effects, in general, and at times even profound results. But it’s not a silver bullet. It’s not a cure all. It’s not for every person or every condition. But it is a tool in the clinical tool chest that some people respond very positively to.
So, how is Cannabis a medicine?
Well, simply put, a lot of ways. There is still a lot we don’t know, but there is a lot we do know regarding the safety of Cannabis and the use of Cannabis traditionally as a medicine for thousands of years throughout human history. While, yes, some of the claims about cannabis as a medicine are over-hyped, a lot of them aren’t. A lot of people are finding relief from very serious conditions that they are having to live with every day through the help of Cannabis.
Today it seems like the rationale for restricting access to Cannabis or Cannabis products often comes down to an argument around safety and a lack of research. Harper Grace is fighting for access to CBD oil because lawmakers in Mississippi feel that Cannabis needs to be studied more to understand its risks. The FDA has stated that they are unlikely to allow CBD in foods because they want to better understand the potential risks.[25] This issue with CBD safety is particularly interesting considering the World Health Organization already issued a report in 2018 claiming “CBD is generally well tolerated with a good safety profile…To date there is no evidence of any public health-related problems associated with the use of pure CBD.”[26] Despite this determination, the FDA backs their stance by citing a recent rodent study that claimed to have identified the liver damaging effects of CBD[27] – however as we covered in episode one of the podcast – this study was a rodent study that utilized massive, unrealistic, doses of CBD before uncovering damaging effects. At doses more typical of what anyone might encounter in real life – these liver damage effects were not observed.
Very recently, democratic presidential candidate and former vice president Joe Biden stated that he believed that there needed to be more research into the risks of Cannabis, particularly as a gateway drug, before legalizing the plant federally.[28] Yet, as we also covered in episode one of the podcast, an administrative law judge in the US in 1988 made a formal statement attesting to the safety profile of Cannabis and the need to reschedule it to a more lenient drug schedule.[29]
So, what do you think?
Do we need more research into the safety of Cannabis before we legalize nationwide? How much evidence is enough before people are allowed open, legal access to Cannabis for medical purposes around the world?
Personally, I was left with a couple of questions:
- Why are Cannabis and its cannabinoids still schedule I drugs in the United States? It’s clear Cannabis has therapeutic applications in certain contexts. Sure, Cannabis can be abused, but so can many other things which are totally legal. Many lawmakers claim we need more research, but how will that research ever take place if Cannabis remains schedule I? Ultimately, the legal status of Cannabis seems to be hurting people more than the plant itself could ever do.
- Given the safety profile of Cannabis, and its potential efficacy, contrasted with the sometimes-harsh effects of some other medications, why is Cannabis often used as a last resort treatment option for patients, rather than one of the early options?
- How much of the benefit that users claim they are getting from Cannabis is actually related to its therapeutic activity, and how much might be placebo? And if some of Cannabis’ therapeutic effects are placebo effects – does that matter, if people are finding relief and the treatment is relatively benign?
So far, we have been looking at the various ways Cannabis is used as a medicine. But what do cannabinoids and other chemicals in Cannabis actually do in the body to elicit these medicinal effects?
Join me in our next episode as we take our fantastic voyage into the human body to understand how Cannabis works. In the next episode we begin to explore the question, “What is the endocannabinoid system?”
Until next time, I’m your host, Jason Wilson. Thanks, and take it easy.
[OUTRO MUSIC]
CITATIONS
[1] https://www.coloradopotguide.com/images/blog/Health-Effects-of-Marijuana-Reduced.png
{kind=link}
[2] https://miro.medium.com/max/1400/0*T-fJXuEjKW4qGUXM.jpg
{kind=link}
[3] Rohrig et al. Types of Study in Medical Research. Part 3 of a Series on Evaluation of Scientific Publications. Dtsch Artztebl Int. 2009. 106(15): 262-268.
[4] Kabisch et al. Randomized Controlled Trials. Part 17 of a Series on Evaluation of Scientific Publications. Dtsch Artztebl Intl. 2011. 108(39): 663-668.
[5] Devlin RB et al. In vitro studies: what is their role in toxicology? Exp Toxicol Pathol. 2005. 57 Supple 1:183-188.
[6] Lorian V. Differences between in vitro and in vivo studies. Antimicrob Agents Chemother. 1988. 32(10): 1600-1601.
[7] Ghallab A. In vitro test systems and their limitations. EXCLI J. 2013. 12: 1024-1026.
[8] Geraghty RJ et al. Guidelines for the use of cell lines in biomedical research. 2014. Br J Cancer. 111(6):1021-1046.
[9] Waterbor JW et al. Considerations of sample size in medical research. JAAPA. 2008. 21(4)
[10] Mullane K et al. Chapter 1 – Reproducibility in Biomedical Research. Research in the Biomedical Sciences. Transparent and Reproducible. 2018. pp. 1-66.
[11] LeFort SM. The Statistical versus Clinical Significance Debate. 1993. 25(1):57-62.
[12] Singal AG et al. A Primer on Effectiveness and Efficacy Trials. Clin Transl Gastroenterol. 2014. 5(1): e45.
[13] https://www.fda.gov/drugs/development-approval-process-drugs
[14] https://www.gwpharm.com/healthcare-professionals/sativex
[15] https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-comprised-active-ingredient-derived-marijuana-treat-rare-severe-forms
[17] https://www.ama-assn.org/delivering-care/public-health/how-are-prescription-drug-prices-determined
[18] Fassbender M. Clinical trial cost is a fraction of the drug development bill, with an average price tag of $19m. 2018. https://www.outsourcing-pharma.com/Article/2018/09/26/Clinical-trial-cost-is-a-fraction-of-the-drug-development-bill
[19] https://www.cnn.com/2013/08/07/health/charlotte-child-medical-marijuana/index.html
[20] https://www.cnn.com/2013/08/08/health/gupta-changed-mind-marijuana/index.html
[21] Rowell N. Harper Grace’s Legacy. North Side Sun. 2019 Apr 11. https://www.northsidesun.com/news-breaking-news/harper-grace%E2%80%99s-legacy
[22] Russo E. The Pharmacological History of Cannabis. Chapter 2. Handbook of Cannabis. Oxford University Press. 2014. p.23-29
[23] Whiting PF et al. Cannabinoids for Medical Use. A Systematic Review and Meta-Analysis. JAMA. 2015. 313(24): 2456-2473.
[24] Hill KP. Medical Use of Cannabis in 2019. JAMA. 2019. 322(10): 974-975.
[25] https://www.fda.gov/consumers/consumer-updates/what-you-need-know-and-what-were-working-find-out-about-products-containing-cannabis-or-cannabis
[26] World Health Organization (WHO). Cannabidiol (CBD) Critical Review Report. Expert Committee on Drug Dependence. Fortieth Meeting. 2018. https://www.who.int/medicines/access/controlled-substances/CannabidiolCriticalReview.pdf
[27] Ewing et al. Hepatotoxicity of a Cannabidiol-Rich Cannabis Extract in the Mouse Model. Molecules. 2019. 24(9): 1694.
[28] https://www.washingtonpost.com/nation/2019/11/18/joe-biden-marijuana-gateway-drug-legalization/
[29] https://www.nytimes.com/1988/09/07/us/judge-urges-allowing-medicinal-use-of-marijauna.html
Podcast: Play in new window | Download (Duration: 48:50 — 45.0MB)
Subscribe: Spotify | Amazon Music | iHeartRadio | Email | TuneIn | RSS | More